

Updated 28th May 2020
By Aida Suarez-Gonzalez1, Gill Livingston2 and Adelina Comas-Herrera3
(with thanks to the Alzheimer’s Society for providing some of the data included in this report)
1Dementia Research Centre, UCL Institute of Neurology at Queen Square, University College London.
2Division of Psychiatry, University College London, UK; Camden and Islington NHS Foundation Trust, London, UK
3Care Policy and Evaluation Centre, Department of Health Policy, London School of Economics and Political Science
Background
In late January 2020, the first COVID-19 cases in the UK were confirmed in North Yorkshire. By the 1st of March, the transmission of COVID-19 within the UK had reached England, Northern Ireland, Scotland and Wales. On 23rd of March, a nationwide lockdown was imposed in the UK. Of all deaths occurring up to 23rd of May in England, 40,096 were confirmed as involving COVID-19 and as 24th of May, 3,779 COVID-19 related deaths were registered in Scotland and 1307 in Wales. However, as COVID testing was not widely available outside hospital this means that many people dying of COVID -19 may have not been registered as such. The majority of COVID-related deaths (around 86%) have been among people aged 65 and over, with 39% of these occurring in the over-85 age group.
A recent report suggests that there around 885,000 people living with dementia in the UK, 85% of whom are living with moderate to severe dementia. 39% of people with dementia over 65 are living in care homes and 61% are living in the community. That report used data from the Cognitive Function and Ageing Study II to estimate the share of people in care homes who had dementia (70%). A more recent study found that an estimated 86% of care home residents in England have dementia. Deaths in April registered as from dementia in England were 83% higher than usual, and 54% higher in Wales.
Effects of confinement to home during COVID-19 lockdowns
Living in confinement may present particular challenges for people living with dementia. Interruption of previously well-established daily routines, reduction in social interaction, particularly with recognised and trusted relatives, and access to vital support services may have a negative impact on both the cognitive function and quality of life of people with dementia and their families, who are also experiencing increasing isolation and inability to access respite care (a, b). At the beginning of April, The Alzheimer’s Society launched an emergency funding appeal to be able to respond better to the thousands of COVID-related calls received since the pandemic started. As per 23rd May the charity stated that around 80% of the thousands of calls they receive were about coronavirus issues and they had an increase of 600% in people joining their online community called ‘talking point’. Moreover, Alzheimer’s Society run a survey among 877 carers of or people living with dementia and found that 78% of people affected by dementia felt more lonely and isolated since the lockdown started and 46% find it hard or extremely hard to cope during the outbreak.
For people living with dementia in care homes, measures to prevent and control infection present particular challenges, as residents are no longer able to receive visits, the normal routines are no longer possible, staff will often wear Personal Protection Equipment (PPE) (which makes recognition and communication more difficult), and many permanent staff may be absent as they are self-isolating. Residents are often asked not to leave their rooms but may not understand why, be restless and so find it hard to stay still and become frightened at being by themselves.
Effects post-lockdown
The effects that prolonged periods of isolation derived from the lockdown may have in people living with dementia in all stages of severity is still unknown. Initial reports have started to be published in the media of people in mild stages declaring feeling less confident and more impaired than before the lockdown.
Risk and consequences of COVID-19 infection
Cognitive difficulties experienced by people living with dementia may make reliable implementation of preventative measures more difficult and can potentially increase their risk of contracting the virus. Besides, people with dementia who develop infections are more likely to develop delirium, which complicates hospital management and compromises the future cognitive health of patients. People with dementia also experience greater functional loss during hospital stays and are likely to experience worse post-discharge functional recovery than those without dementia.
There is no certain evidence that dementia itself increases the risk of COVID-19 infection or necessarily compromises the chances of survival in case of infection (except perhaps in very advanced cases). However, COVID-19 symptoms and death rates increase with older age and with pre-existing illnesses such as cardiovascular disease and diabetes. As people who have dementia are more likely to be older and have underlying health conditions, and to live in a communal setting, this puts them at higher risk of developing severe complications from COVID-19.
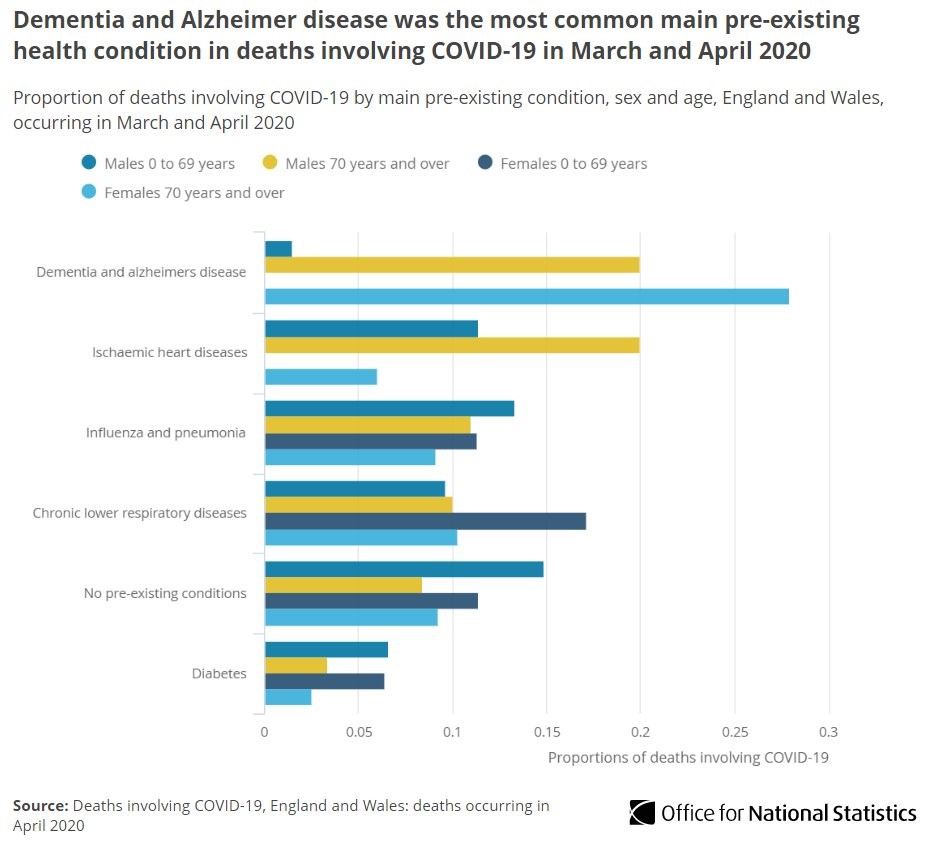
The Office for National Statistics (ONS) found that 20.4% of COVID-19 related deaths that occurred in March and April 2020 in England and Wales were in people whose death certificates also specified they had dementia and that dementia were the most common underlying health condition (see Figure below).

Recent research from the University of Exeter and the University of Connecticut from the UK biobank (available in preprint) found that the 448 COVID-19 patients aged 65 or older in the biobank were three times more likely to have pre-existing dementia than the others in a the cohort. It is unclear though whether this corresponds to the fact that more people with dementia contracts the virus or because people living with dementia develop more severe clinical pictures of COVID-19 that require admission to hospital (only hospital in-patients with clinical signs of infection included in the COVID-19 sample). It is important to consider whether the high share of people with dementia living in care homes, where the difficulty in implementing physical distancing measures is well documented, may have been a factor.
Another recent study by Bianchetti et al., (2020) have described a mortality rate of 62% among COVID + patients with dementia compared to 26% in COVID + patients without dementia. Although this higher mortality rate may be in principle attributed to the older age of people living with dementia and severity of the dementia, the authors also found that the mortality rate of people with mild dementia (presumably younger and fitter than those with severe dementia) was 41%, and therefore still significantly higher than the mortality rate for those without dementia.
Risk of becoming infected and dying in care homes
In the UK, as in many other countries that have experienced rapid surges in COVID-19 infections, there have been large numbers of deaths linked to COVID-19 among care home residents.
We calculated mortality of people with dementia based on the estimate that 86% of people living in care homes in the UK have dementia, and assuming that people in care homes with dementia have the same probability of dying from COVID-19 as residents without dementia (which is still unclear since more comorbidity is often present in those with dementia and we are unclear if dementia is in itself a risk factor). In England, out of the 15,414 COVID-19-related deaths of care home residents reported to the Care Quality Commission between the 10th April and the 22nd of May, 13,256 would have had dementia.
On 13th May, Alzheimer’s Society reported that 43% of care homes surveyed by the charity the week before declared they felt still unconfident about their PPE supply, with one of the care homes still resorting to plastic bags as a form of PPE. 58% of the homes questioned said there were unable to isolated residents, in particular those living with dementia. Care home operators have also reported a lack of systematic testing in care homes and they have told the media that are getting continued confusing messages from Public Health England (PHE) and the Care Quality Commission (CQC), with each public body passing the responsibility of care home testing to the other.
The Alzheimer’s Society is also campaigning for daily data from care homes to be collected so that the public, care providers and authorities can have a better picture of the scale of the impact of COVID-19 and adjust timely and realistic responses. This is particularly important for people living with dementia, who comprise most of the residents care homes in the UK, and who show more atypical presentations of COVID-19 infection and may be at a higher risk of death if contracting the virus. Moreover, an investigation of COVID-19 outbreaks in London (Graham et al., 2020, awaiting peer-review) found that 43% of all COVID positive residents were asymptomatic and 18% showed atypical symptoms, so acting only with those with typical symptoms is likely to contribute to spread of the virus.
Ensuring access to health care: admissions to hospital and Intensive Care Units
On the3rd of April there were media reports that the local Clinical Commissioning Group had circulated a document to GP practices and nursing homes in Brighton and Hove stating that many vulnerable people may be refused admission to hospital. They directed all homes to check whether they had resuscitation orders about every resident. Care home managers in the area expressed concerns about residents and families being pressured into signing these forms, one care home reported having 16 residents out of 26 sign do-not-attempt to- resuscitate (DNAR) forms in one day. Likewise, care home managers in Greater Manchester complained about care home residents being refused hospital treatment and DNAR orders being issued about residents without consulting with their families. It is unlikely that many of those residents were able to understand and make a judgement about what they were signing because of their cognitive impairment. In these cases where the residents lacked capacity but their relatives were not consulted about their best interests, the forms would have been illegal.
Care home providers in York also claimed that hospitals were refusing to admit COVID-positive residents. A GP surgery in Wales apologised after sending letters recommending its more vulnerable patients to complete DNAR forms to ensure that emergency services would not be called if they contracted COVID-19. In addition, care home beds were being blocked booked to free up hospital beds and new residents admitted with unknown COVID-19 status. When a resident moves into a home with unknown and sometimes asymptomatic COVID-19 they may potentially infect a large number of residents and staff. This reservoir of infection is not only a risk for the residents but would be expected to feed back into the community as the staff go home after their shift.
The Alzheimer’s Society echoed similar concerns: ‘Every day our Dementia Connect support line hears from people, friends and families terrified about the impact of coronavirus – people with dementia are being abandoned in care homes. They’re being told they won’t be admitted to hospitals, they’re being asked to sign DNAR orders and being discharged from hospitals to care homes without being tested”. An open letter sent by the Alzheimer’s Society and 4 leading charities to health secretary Matt Hancock about people living in care homes sates that people with dementia in care homes “are told they cannot go to hospital, routinely asked to sign DNR orders”.
DNAR orders are intended to be issued to prevent pointless suffering from resuscitation that will not be of benefit. These orders and advanced care plans about refusal of care are appropriate for some older people with dementia and other illnesses, who may be distressed by admission to unfamiliar places with little expected benefit. In those with severe dementia, any attempt at resuscitation is very unlikely to lead to a good outcome. The use of DNAR, and whether it would be in someone’s interest to be admitted to hospital, should be considered carefully, in advance of the decision needing to be made. These orders should only be issued after discussions have been held with the persons or if they lack cognitive capacity to consent with their families, a practice incompatible with mass signing.
The struggles of some Intensive Care Units (ICU) to cope with the increasing number of admissions was already reported before the announcement of the lockdown, with some hospitals experiencing a thirteenfold increase in patients before 20th of March, and testimonies of doctors on the 3rd April describing how the criteria to access ventilation were becoming so strict that “soon many of our own staff would not meet criteria”. The National Institute for Health and Care Excellence (NICE) published COVID-19 guidelines for critical care in adults along with a critical care referral algorithm. For people over 65, this algorithm recommends the use of a Clinical Frailty Scale (CFS) score. Individuals obtaining a CFS score of 5 are classified as frail and, according to the guidelines, “there is uncertainty regarding the likely benefit of critical care organ support”. In principle, as it specifically mentions dementia, although no other illness, all people with dementia would be immediately included in this frail group (including people with mild Alzheimer’s disease, who may have more than a decade of life expectancy ahead of them). Although NICE stipulates that this CFS score is part of an holistic evaluation, it is unclear how this algorithm would be used when resources are scarce and doctors have to face rapid life-death decision.
This led Alzheimer’s Society to make a call for the NICE to clarify how clinicians will judge a ‘positive outcome’ for people with dementia when making clinical decisions for admission to ICU and assurance that the use of the CFS will not disadvantage people with dementia with regards to access critical care at a time of insufficient resource. The Lewy body Society also sent a letter to the Health Secretary expressing their concerns about people with dementia with Lewy body being at disadvantage if current CFS is used on them. Access to hospital or critical care has not been guaranteed in general for people living with dementia in the UK.
There also appear to have been difficulties for care home residents to access primary care. The Alzheimer’s Society survey of care home managers also revealed that 75% of 104 care homes that responded to the survey said GPs have been reluctant to visit residents and 51.92% are having to verify the cause of death because GPs are not visiting
Measures to support people living with dementia during the pandemic
Clinics by phone or videoconference
Specialised clinics and liaison with specialist for acute hospitals and care homes for people living with dementia continue over the phone or by videoconference. For those at very high risk because of symptoms of the dementia, specialist staff may visit wearing PPE.
Measures to support people with dementia in hospital
NHS England published guidance banning hospital visits to prevent the spread of the virus. However, people living with dementia were later included under the list of exceptional circumstances where one visitor would be permitted to visit.
Measures to support people with concerns about the lockdown measures or COVID-19
The third sector is a point of reference of support for people with dementia in the UK. The NHS website signposts people with dementia concerned about COVID-19 and the lockdown measures to the pages of the leading dementia charities Alzheimer’s Society and Dementia UK for advice. Both organisations launched COVID-19 sections in their websites early on and continued their support services through the lockdown. Rare Dementia Support, a UCL-led charity aimed at providing support to people with less prevalent forms of dementia also launched a COVID-19 emergency kit and new services during the pandemic. The Lewy Body Society has campaigned for the rights of people living with dementia with Lewy body (DLB) and raised concerns to the Health Secretary about the possibility that pressures on the NHS and health workers may “mean greater use of drugs to treat people with DLB rather than the non-pharmacological treatments that are usually recommended”. Some professional societies, like the British Geriatrics Society, have also published guidance to support people living with dementia during the pandemic.
Many activities to support people living with dementia that were already running across the country, migrated to online mode to continue providing support, as for instance the Ely’s dementia choir, the Alzheimer’s Society Singing for the Brain and the music therapy group Together in Sound.
Measures to maintain community-based long-term care services
An estimated 60% of people receiving home care services in the UK are people living with dementia. The UK government issued guidance on home care provision for local authorities, clinical commissioning groups and registered providers during COVID-19. Additional guidance on the safe use of PPE for domiciliary care workers was published on the 30th April. This guidance includes the responsibility of home care providers to routinely procure personal protective equipment (PPE). However, the United Kingdom Homecare Association (UKHCA) warned that the spiralling price of PPE, among other financial pressures, may lead to many firms to close and thousands of isolated vulnerable people being left to without care services. The government announced funding to support the sector but on the 29th April, UKHCA’s CEO declared to that home care providers were unable to source stocks from the supply chain. On the 3rd May 2020, the lack of PPE among home care workers remained a widespread problem. On 22nd of May, the UK government issued guidelines about the provision of home care during the COVID-19 situation, including advice in relation to getting the right PPE.
Measures to support residents in care homes
In a number of dementia care homes the staff have voluntarily moved in with their residents to shield them from the virus. An increasing number of care homes are beginning to explore options to make visits by family members safe, recognizing the distress that not being able to see their families is causing to many people who live with dementia in care homes.
Concluding remarks
Health and care workers and third sector organisations continue playing a very important role in supporting and protecting the rights of people living with dementia during the crisis in the UK. Concerning practices of refusing admission to people living with dementia to hospital, lack of antigen testing of those either living or working on care homes, or those moving in, a lack of PPE in care homes and mass signing of DNAR forms have been reported by different media sources and in different geographical locations across the UK. Professionals and the voluntary sector have spoken out about the effects and are working to mitigate them. Emerging evidence is raising questions about the very high vulnerability of those living with dementia to serious illness or death from COVID-19 and that may remain under-recognise. Effects of prolonged lockdown or post-COVID hospital discharged need further investigation. Dementia care in the UK has been negatively impacted at many levels by the COVID-19.
Note: Much of the information in this report has been gathered from media news and official reports. If you notice any inaccuracy, please email aida.gonzalez@ucl.ac.uk